
How to support the health and wellness of female physicians
A recent CMA study found that 54% of physicians in Canada under the age of 40 are women. By 2030, women are expected to make up half of all physicians in Canada. Yet many women in medicine continue to face challenges including pay and leadership inequality, sexual assault and harassment, opposition to career advancement, gendered stereotypes, unfair role expectations, and unconscious bias.
These challenges are amplified for women who also belong to a racial or religious minority, low socioeconomic demographic, 2SLGBTQIA+ community or disabled population.
In a CMA survey of female physicians and medical students at the 2020 Canadian Women in Medicine Conference,
77% said they had experienced gender inequity in their training or practice setting, and 99% reported that the inequity had a negative effect on their sense of wellness.
At the same time, 83% said their workplace does not offer any organizational practices, programs, policies or resources to support women in medicine.
The high cost of gender bias
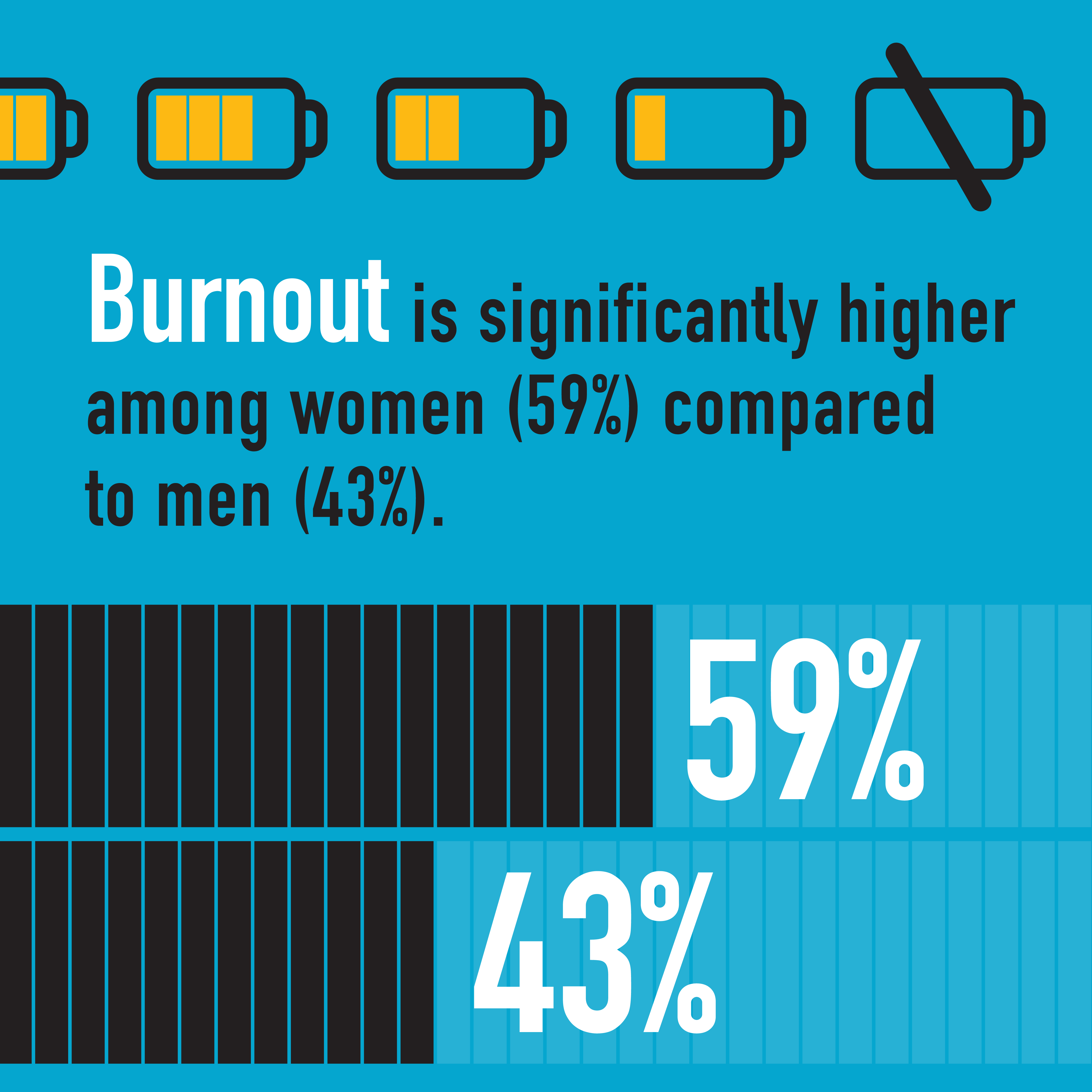
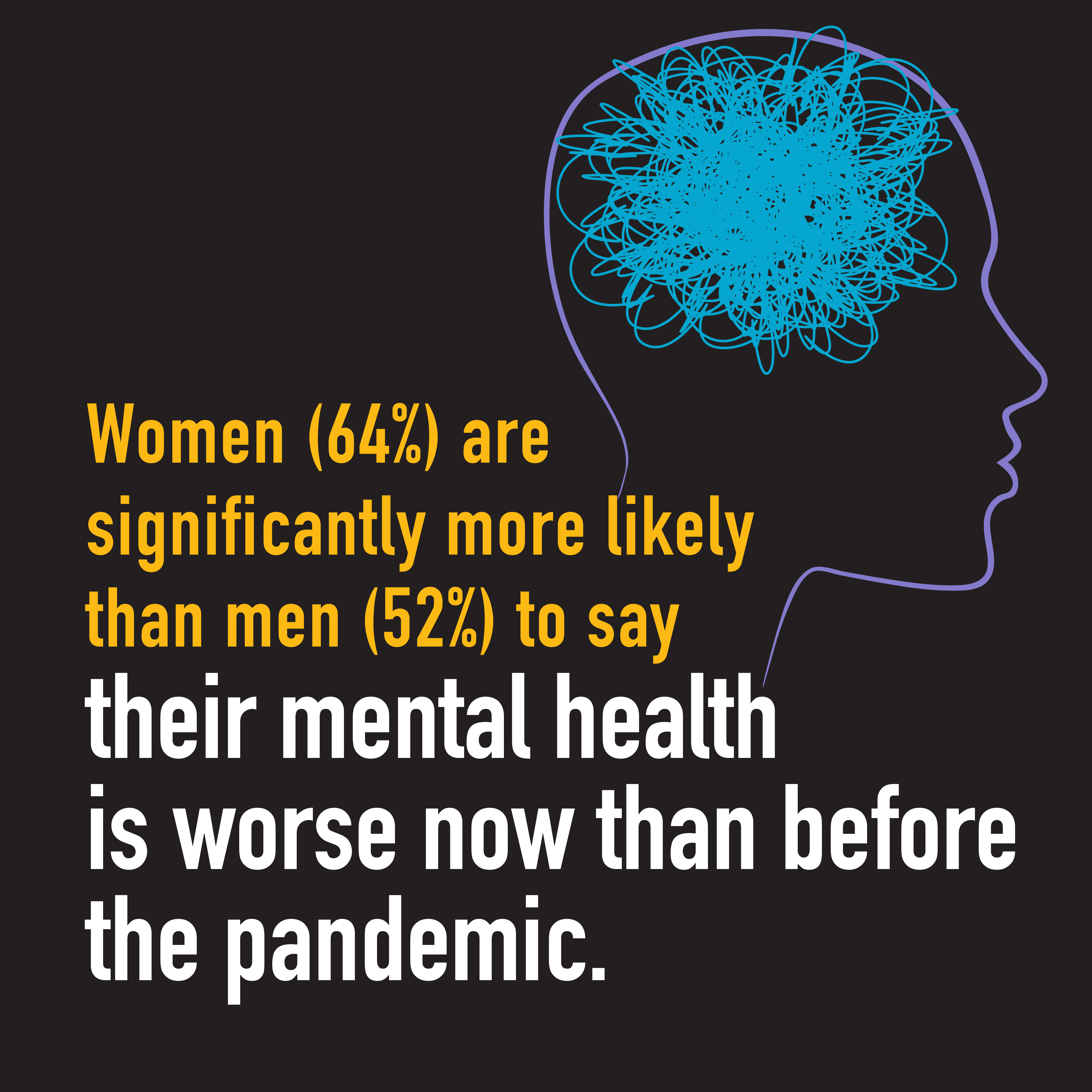
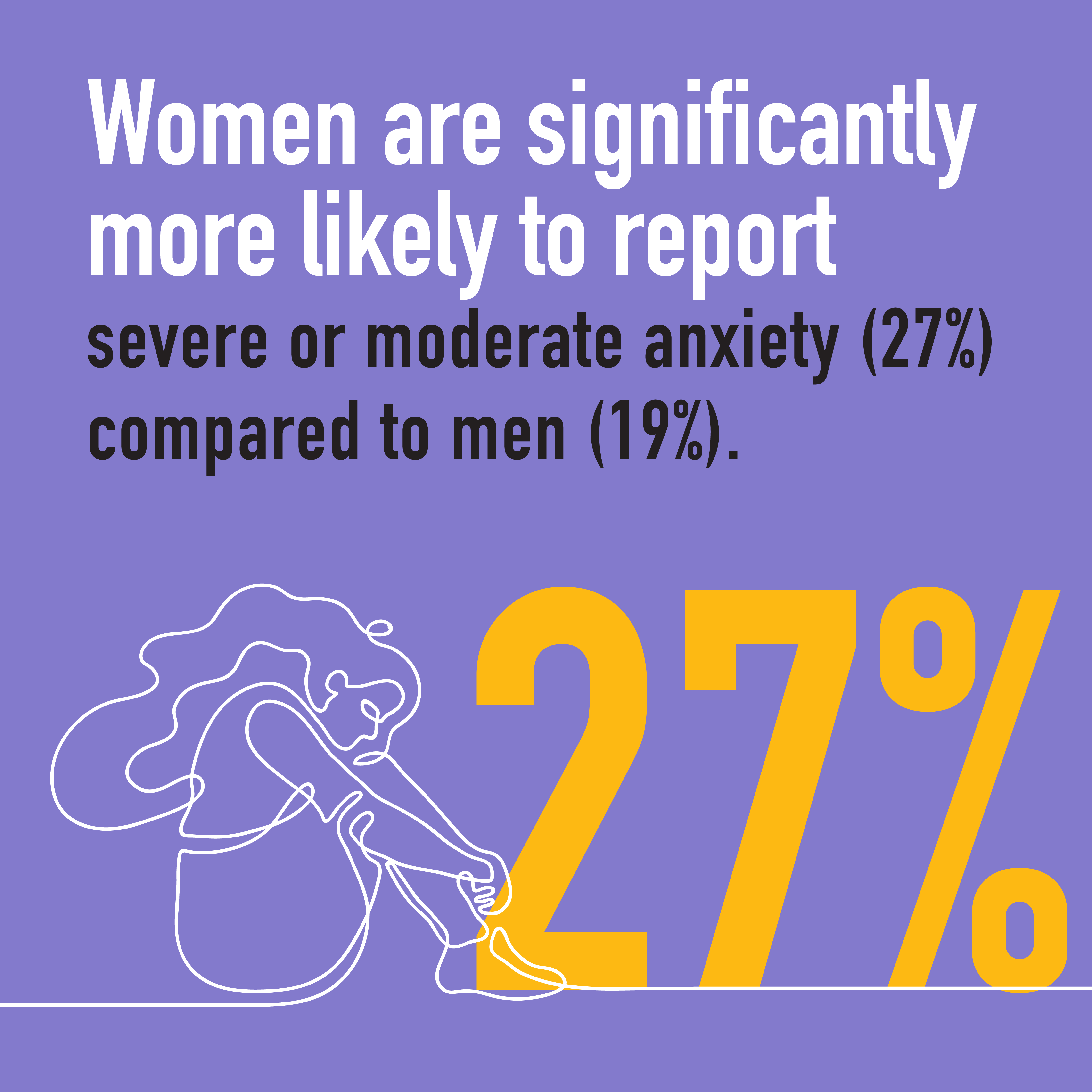
Gender bias is often unintentional and even unconscious, but it can have a very real negative impact on female physicians. In more than 2,300 responses to the CMA’s 2021 National Physician Health Survey, female physicians are reporting higher levels of burnout, anxiety and harassment in the workplace compared to their male peers.
The positive impacts of including women in medicine
An equitable and diverse medical population delivers better patient care and a more responsive, adaptable health care system by contributing different points of view and providing underserved populations with better access to medical services. It also improves physicians’ career satisfaction, health and wellness, and builds solidarity within the profession.
Women physicians usually spend about 10% longer with patients and communicate more effectively, resulting in 6% fewer visits per patient. Women also tend to emphasize preventive medicine more than their male colleagues, allowing for earlier detection and intervention.
Women physicians are also often effective disruptors who can improve the system overall — for example, by leading advocacy for greater work-life integration and inte¬gration of care through multidisciplinary teams.
Individual and systemic solutions for achieving equity
Confronting inequity and achieving equity in medicine is a shared responsibility that calls for action at both the individual and system levels.
Systemic changes for leaders at medical organizations and institutions
- Review all policies, procedures and practices with an equity and diversity lens. This review should look at:
- Recruitment
- Hiring
- Pay
- Promotion
- Leaves of absence
- Parental leave
- Resources and support
- Working/learning conditions and accommodations
- Provide platforms, resources, education and training to effect change collaboratively. Train staff in implicit bias, allyship, cultural safety and humility, cultural and structural competence, and the value of diversity in improving health outcomes.
- Provide leadership continuous improvement through feedback and evaluation of policies and programs.
- Make sure women who experience discrimination, harassment or abuse have safe and effective ways to report it outside of their supervisory/promotional chain, and ensure they can seek counselling without fear of negative consequences.
- Promote and enable formal and informal mentorship and sponsorship opportunities for under-represented groups.
- Promote and foster decision-making environments where diverse perspectives are solicited, heard and appreciated.
- Seek research and funding opportunities to encourage the collection and use of equity and diversity data and, specifically, review data practices to ensure:
- Historically under-represented groups are meaningfully engaged
- Data on under-represented groups is appropriately collected and analyzed
- Information collected is used to inform internal policy and practice to reduce or eliminate system-level drivers of inequity
- Findings related to this data are made accessible
Individual behavioural changes
- Make a personal commitment to recognize others as equals.
- Cultivate respectful, open and transparent dialogue and relationships.
- Support colleagues in meeting their individual and collective responsibilities to their patients and colleagues.
- Follow the principles that guide the medical profession, and respond justly and decisively when you see these principles being ignored.
- Advocate for equity and diversity to achieve equitable health outcomes.
Case study: An equity-building initiative
The University of California Davis School of Medicine established its Women in Medicine and Health Science (WIMHS) Program in 2000 to ensure the full participation and success of women in all roles within academic medicine and science. As part of this initiative, UC Davis worked with the Association of American Medical Colleges (AAMC) and other medical schools to advocate for women’s advancement and leadership in education, research, clinical practice and administration. It promoted strategies to enhance and sustain a climate of inclusion, equity and opportunity. It also collected, analyzed and applied data to inform institutional and individual decisions and actions.
The school developed and disseminated a number of initiatives and resources, including mentoring and career development programs, while also providing opportunities for networking. Finally, the program made sure to recognize and celebrate women’s accomplishments.
The WIMHS Program received enthusiastic support from faculty and school leadership, and contributed to the development of strong internal parterships. As a result of the initiative, UC Davis saw a steady increase in the number of female faculty and department chairs and experienced a relatively low departure rate for female faculty (34% vs. the 40% national rate reported by the AAMC that year).
Results from the latest 2021 National Physician Health Survey and more recent physician health and wellness data are available here.
Topics
Are you in distress? Get help now.