Synopsis
The CMA surveyed e-Panel members to inform the association’s submission to the federal Task Force on Marijuana Legalization and Regulation. As the federal government prepares to introduce legislation for spring 2017, physicians answered questions that provided insight into their concerns and opinions about marijuana distribution, consumption, regulation and supports required for frontline practitioners. A summary of the results of the e-Panel survey is presented below.
Survey – July 2016
The survey was sent out to 4, 244 e-Panel members; 788 responded, for a response rate of 18.57%.
Results
Federal regulatory regime
When asked about the regulatory regime that the federal government will implement for recreational (non-medical) marijuana use, 43% of respondents supported a single system for regulating both marijuana for medical and recreational uses. About the same proportion (39%) supported creating a second regulatory system for non-medical use, separate from that of marijuana for medical purposes.
When asked for suggestions for changes to the regulation of marijuana for medical use, the main themes that respondents provided were as follows:
- Regulating and standardizing dosages, strains, THC/CBD concentrations;
- Funding research focused on other intake methods of marijuana;
- Further government-funded research on the benefits harms associated with marijuana;
- Providing physicians the choice to authorize marijuana or not;
- Providing physicians with guidelines for authorization of marijuana for cases they deem necessary (minimum age of patient, evidence-based resources);
- Improving the availability of marijuana to patients while restricting its accessibility to youth; and
- Having insurance coverage for marijuana for medical purposes.
Marijuana distribution for non-medical use
When asked about their preference for distribution models for recreational use, participants responded as follows:
- 56% agreed or strongly agreed with distribution through existing non-health care structures (e.g. liquor stores or similar);
- 47% agreed or strongly agreed with distribution through legal storefronts, specifically for the sale of marijuana (e.g. independent dispensaries);
- 29% agreed or strongly agreed with distribution through a health care setting (e.g. pharmacies);
- 16% agreed or strongly agreed with distribution through mail, as is currently done with marijuana for medical purposes.
There was not a clear consensus on whether provincial and territorial governments should be left to decide on appropriate distribution mechanisms (35% agreed or strongly agreed; 40% disagreed or strongly disagreed).
Respondents’ comments on the various possible distribution models included the following:
- Need for supporting distribution models through effective staff training, offering education and counselling support for users;
- Providing ease of access, regulating sales, impromptu inspections;
- Restricting access to minors and other vulnerable populations;
- Treating distribution of marijuana for recreational use similar to the alcohol distribution systems in place; and
- Government-controlled prices and taxes for licensed dispensaries.
Personal growth of marijuana plants for non-medical use
When e-Panel members were asked about the extent of agreement in allowing people to grow their own marijuana plants, about 40% of respondents agreed or strongly agreed with this option.
Respondents’ comments on allowing personal growth of marijuana plants included the following:
- Allowing growth but for personal use, not commercial;
- Allowing to grow small/limited amounts at home;
- Enforcing certain parameters, following housing codes and hazard protocols;
- Preventing young children, minors, pets from accessing home-grown marijuana plants; and
- Lack of product control and regulation, pesticide use.
Locations for consumption of marijuana for non-medical use
Respondents were asked about where people should consume marijuana for recreational use. Nearly 80% of respondents preferred consumption in private homes, and only 36% agreed with marijuana consumption in designated public places.
Respondents were split on whether the same consumption places should be used for marijuana use as for tobacco smoking, with 43.0% agreeing and 43.2% disagreeing.
When we asked respondents for their comments on the locations to consume marijuana recreationally, major themes raised included:
- Concerns about second-hand smoking in open public places; and
- Concerns about exposing minors to marijuana smoke.
Minimum age for purchasing and possessing marijuana for non-medical use
When respondents were asked about what minimum age the government should adopt for purchasing and possessing marijuana for recreational use, 25% of respondents recommended the minimum age to be 21 years old.
When prompted about why e-Panel members chose those particular ages, most cited reasons such as:
- Decreased likelihood for psychosis to emerge;
- Adverse effects on the developing/adolescent brain;
- Societal views of being mature at those ages, taking responsibility for actions;
- Allowing marijuana purchasing and possession to occur at the same age as alcohol-use & tobacco-use;
- Age of majority according to the province/territory.
Regulation of THC levels (potency) in marijuana for non-medical use
72% of respondents agreed or strongly agreed with having the federal government regulate THC levels in marijuana for recreational use.
Patient interactions and resources
Excluding those not in clinical practice, 60% of respondents always or often asked their patients about their recreational marijuana use.
Excluding those not in clinical practice, 47% of respondents felt they had the information needed to advise patients on the risks associated with recreational marijuana use. Almost 40% of respondents felt that they did not have the information to adequately counsel patients.
When asked about what other tools would support their practice with regards to marijuana for recreational use, e-Panel members responded that they could benefit from the following:
- Updated information on the research associated with the harms of marijuana (87%);
- Guidelines to counsel patients on marijuana use and driving/operating dangerous equipment would be beneficial for their practice (80%);
- Access to data on the surveillance of the harms of marijuana use e.g. emergency room cases, deaths, hospitalizations (72%);
- Clinical guidelines for the screening and monitoring of chronic users of marijuana (71%).
Within the past year, 18% of respondents authorized marijuana for medical purposes to their patients at least once.
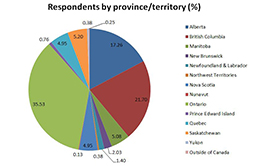
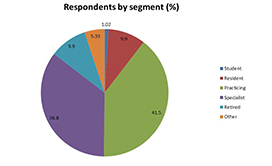
Respondent profile
Next steps
The CMA will continue to engage with the federal government throughout the development of legislation and regulations for marijuana for non-medical purposes, and will continue to represent physicians’ views on this important issue.
Respondents told us
“As physicians we really need a lot more education on this topic.”
“The regulatory framework needs to be able to be adjusted based on the research of the impact, so the law can be more generic and the regulations more specific. There should be a lot of funds allocated to education, de-normalization in youth especially, and to research. Clear regulation will help enforcement, and mechanisms to facilitate citizen's participation in the information needed for enforcement will be helpful.
“CMA must lead on making risks of marijuana use well known to physicians, public and politicians. Must insist on national surveillance data on impacts marijuana use is having on our citizens and society. We must NOT relive the tobacco tragedy.”
“I appreciate the CMA reaching out to membership like this, and am glad that the dialogue is opening up regarding marijuana. I think it will find its place in society just like other prescription drugs and alcohol. I think it has potential harms and benefits, and those should be weighed on a case by case basis, rather than blanket bans or completely unrestricted use. More research would definitely be helpful in determining its clinical applications.”