The CMA’s Act of Incorporation and Bylaws (last amended in August 2022) set out the objects of the association and its governance parameters. In advance of the Annual General Meeting (AGM) on May 29, 2024, we are consulting members on several minor proposed bylaw amendments. These include proposed changes to:
- strengthen and modernize the eligibility criteria for CMA board directors;
- affirm members’ autonomy in applying for leadership positions; and
- clarify AGM notices in the digital age.
If you have any feedback on these proposed changes, please register to attend the governance information session on Apr. 30, or join the ongoing discussion on CMA Community. (Please note: You must be logged in with your cma.ca credentials to participate.)
Strengthening and modernizing the eligibility criteria for CMA board directors
Under the CMA bylaws, the current eligibility requirements for board director candidates are: (i) CMA membership (except the non-physician position); (ii) adherence to the Conflict of Interest Guidelines; and (iii) residence in Canada. There is an additional requirement that the president-elect (who sits on the board of directors) must have been a CMA member for five consecutive years preceding their nomination.
Proposed bylaw amendments for 2024 would require board director candidates to, in addition to the foregoing requirements: (i) be at least 18 years of age; (ii) not have been declared incapable by any court; (iii) not have the status of an undischarged bankrupt; and (iv) not have been found guilty of an indictable criminal offence for which they have not been pardoned.
Why: These requirements are best practice in Canada and explicit under laws that govern most corporations. In contrast, the CMA is governed by its own Act of Incorporation, which does not include the proposed requirements. The CMA recommends a bylaw amendment to make these best practice requirements explicit.
Affirming members’ autonomy in applying for leadership positions
In 2022, members approved bylaw amendments that enabled members to directly apply for leadership opportunities, and the CMA to select its own leadership rather than accepting nominees put forward by the provincial/territorial medical associations and affiliate organizations. The CMA continues to work closely with partner organizations to promote leadership positions.
The proposed bylaw amendments for 2024 would clarify that candidates must submit their application forms directly to the CMA. In addition, references to nominations by third party organizations (e.g., affiliates) or their members would be removed (note: Resident Doctors of Canada no longer has individual members). Finally, since leadership candidates are no longer nominated by a provincial/territorial medical association or affiliate organization, language throughout the bylaws would be updated to replace the term “nominee” with “candidate” or “applicant” where appropriate to ensure consistency.
Why: These proposals affirm existing practices and provide greater clarity and transparency for members and partner organizations.
Clarifying AGM notices in the digital age
The proposed bylaw amendments for 2024 clarify that electronic notice of the AGM (i.e., an email to members and publication on the CMA website) fulfills the existing bylaw requirement that the time and place of the AGM must be announced to members “in an Association publication with distribution to all members.”
Why: These proposed changes affirm existing practice.
The CMA is continuing to explore other governance themes, including who’s entitled to vote for CMA president-elect. Members have provided feedback on this theme through a governance survey in May 2023 and at an information session and through informal polling at the 2023 AGM. If future bylaw changes are put forward in this area, members will have the opportunity to review proposed amendments in advance of the AGM.
Who’s entitled to vote for CMA president-elect
History of the CMA presidency
The CMA has had a president since 1867. As the association has evolved, the role of the president has as well. Beginning with a focus on presiding over the AGM, the role of the president has expanded to focus on being a spokesperson: bringing relevant issues for physicians across Canada to the national stage through government relations, speaking engagements and traditional and social media.
Year |
Role of the president |
Province/territory of the president and the electorate
|
|
1867 |
The president role was established at the first meeting of the association. |
Starting in 1867, the president was selected from the province or city in which the next annual meeting was to be held (the president-elect took office as president when the annual meeting was held in their home jurisdiction). They were elected by all members at the annual meeting. |
|
1868 |
The president role was defined as presiding at meetings and preserving order and decorum during debate. |
|
|
1870 |
In 1870, the president started to be elected by General Council (a subset of members) at the annual meeting. |
|
|
1909 |
The president was appointed as an officer of the association (responsible for presiding at meetings and delivering the annual presidential address during the AGM). |
|
|
1960 |
In addition to presiding at the AGM and delivering the presidential address, the president acquired a new role: “to preside at all social functions of the association.” |
|
|
1983 |
In 1983, a presidential rotation of three 9-year cycles (total of 27 years) was established on the basis of relative membership size in four regions (West, Ontario, Quebec, Atlantic) and the desire to hold the AGM in all parts of Canada. |
|
|
1995 |
The bylaws were amended to recognize the president as the “spokesperson for the Canadian Medical Association” and a spokesperson policy was established. |
|
|
2009 |
In 2009, the presidential rotation was changed to a model of representation by population (one 19-year cycle) that aligned with the number of CMA board members and their provinces/territories (the board had one director per 6,000 members in their jurisdiction). |
|
|
2018 |
In 2018, a proposed bylaw amendment to move to a national president-elect election did not receive the necessary two-thirds majority of support from members to pass. |
|
|
2019 |
In 2019, members approved bylaw amendments to discontinue nominations from the floor at General Council and the ability for five delegates to nominate a president-elect candidate on the first day of General Council. |
|
|
2020 |
In 2020, the presidential rotation was changed to a 12-year alphabetical model across the provinces and territories (except for Nunavut). The CMA began referring to General Council elections as a “ratification vote.” |
|
|
2021 |
In 2021, a proposed bylaw amendment to move to a national president-elect election did not receive the necessary two-thirds majority of support from members to pass. |
|
|
Today |
As the voice of Canadian physicians, the president is a sought-after presenter and speaker across the country. |
The president-elect is elected by members in their province or territory and then approved by General Council delegates at the AGM. |
President as CMA spokesperson
The CMA presidency is currently a three-year term:

President-elect
- Assists the president with spokesperson duties
- Serves as a director on the CMA Board of Directors
President
- Acts as primary spokesperson of the CMA
- Serves as a director on the CMA Board of Directors
Immediate past president
- Assists the president with spokesperson duties
- Serves as a director on the CMA Board of Directors
- Acts as a chair of the CMA Nominations Committee
The role of the CMA president as spokesperson has involved an increasing number of speaking engagements, media appearances and meetings with government. The CMA president also has significant engagement on social media, amplifying the CMA’s advocacy.
Over the past three years, the activities of the president during their year in that role have included, on average:



The online presence of the president via the CMA’s social media channels currently includes:
![]()
~75K followers
![]()
~25K followers
![]()
~70K followers
![]()
~20K followers
The election process
Every year, the CMA issues a call for nominations for the president-elect position in a province or territory according to an alphabetical rotation. Members in that province or territory then elect a CMA president-elect nominee from among the candidates who apply. The electorate ranges from fewer than 100 current members in the Northwest Territories to nearly 14,000 current members in BC (note: Nunavut is not part of the presidential rotation).
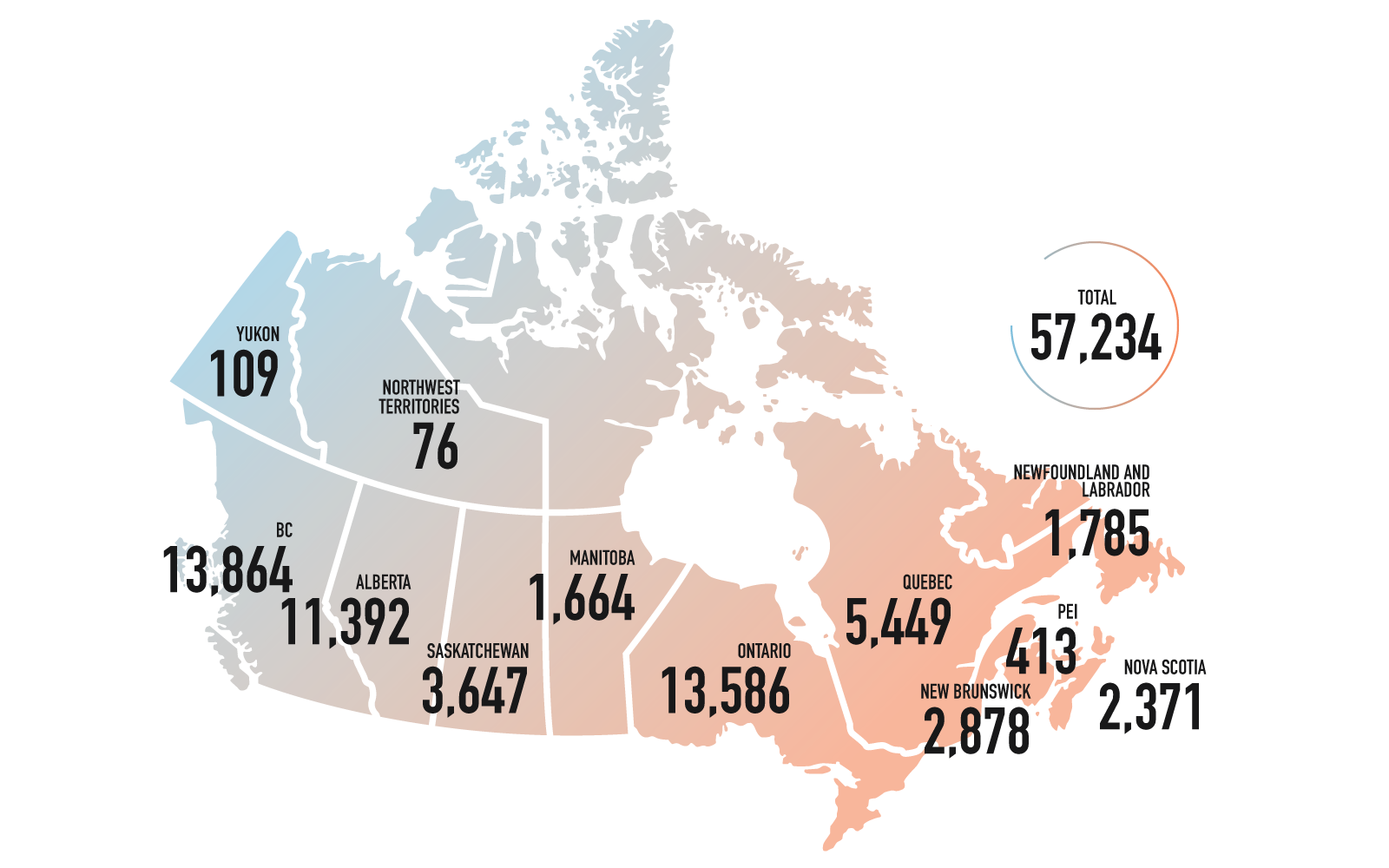
Number of eligible voters (as at December 2022)
Below is the participation rate in the past four president-elect elections:
Year |
Jurisdiction |
Number of eligible voters
|
Total votes counted |
Voting rate |
| 2020 | Yukon | 104 | 78 | 75% |
| 2021 | Alberta | 14,563 | 2,157 | 15% |
| 2022 | British Columbia | 15,105 | 1,510 | 10% |
| 2023 | Manitoba | 1,811 | 773 | 43% |
President-elect approval
The president-elect nominee chosen by the voters in the eligible province or territory is presented for approval by a national body of General Council delegates at the AGM (in 2022, General Council comprised 125 people). In the smaller provinces and territories, the national body of General Council delegates may outnumber the voting membership by 50% to 100%. In larger provinces and territories, the number of General Council delegates may be far smaller than the number of voting members (less than 1%). For example, in 2021, the president-elect electorate in Alberta was more than 14,000 members; the approval vote comprised 118 General Council delegates, 29 of whom were from Alberta.
1 General Council delegates who ratify the elected nominee are defined in the CMA bylaws and include the following: chair of the board of directors; board directors; AGM chair/speaker; AGM vice-chair/deputy speaker; president of each provincial/territorial medical association; members from Quebec who are invited by the CMA to act as delegates; chair of the Committee on Ethics; chair of the Governance Committee; chair of the Awards Committee; a delegate from the Royal Canadian Medical Service, at the direction of the Surgeon General; past presidents (for the previous five years); past chairs/speakers of the AGM (for the previous five years); and past chief executive officers (for the previous five years); and provincial/territorial and affiliate society delegates appointed by their respective provincial/territorial medical association or affiliate society.